Heel Pain That Won’t Go Away? As a Clinician, I Know It’s Not Always Plantar Fasciitis

One of the most common foot complaints I encounter is persistent heel pain. In many cases, the diagnosis is quickly labeled as plantar fasciitis — and often, that’s correct. But clinical experience and growing evidence remind us of an important truth:
Heel pain that doesn’t respond to standard treatment is not always plantar fasciitis.
Mislabeling heel pain can lead to prolonged symptoms, patient frustration, and inappropriate management. Understanding the full differential diagnosis is essential.
Plantar Fasciitis: Common, but Frequently Over-Assumed
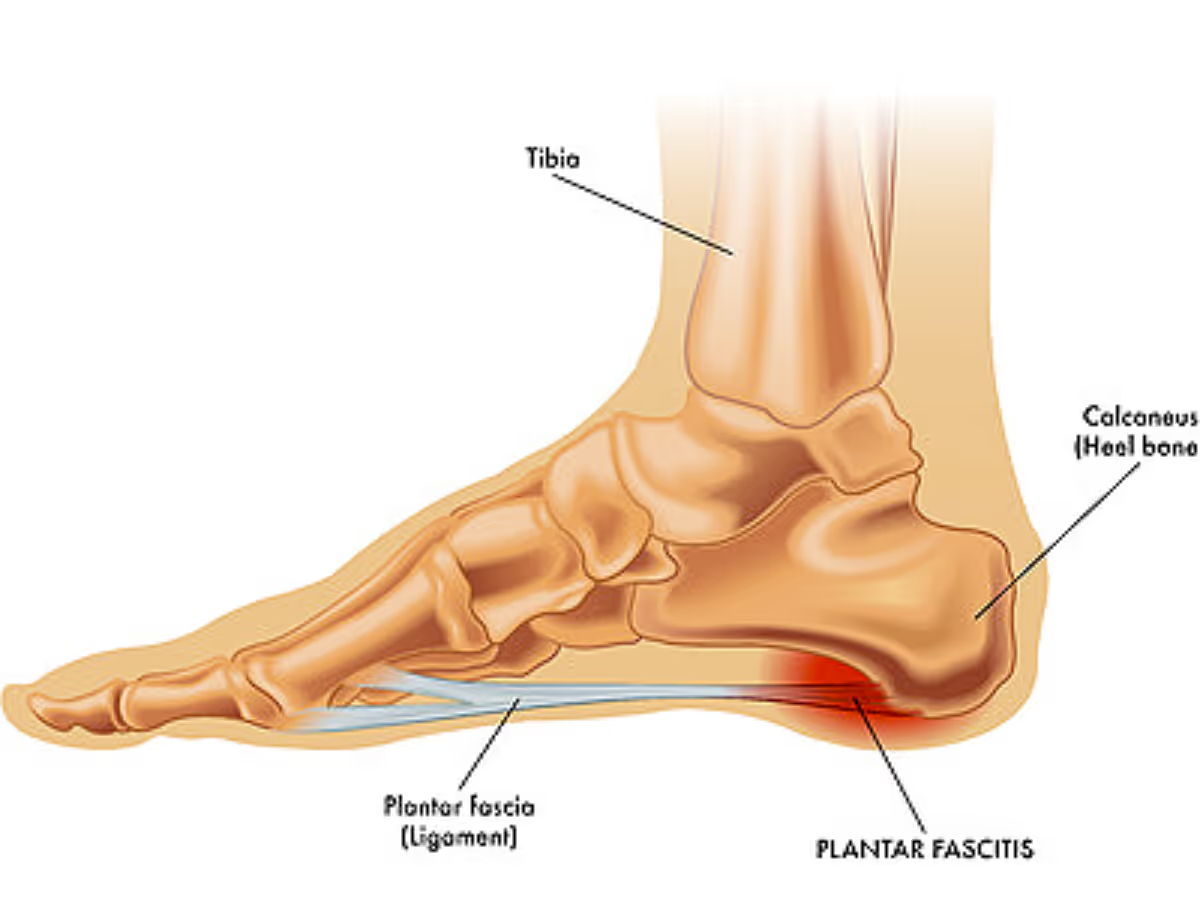
Plantar fasciitis (more accurately termed plantar fasciopathy) is now understood as a degenerative overuse condition, not a primarily inflammatory one. Histopathologic studies demonstrate collagen disorganization and microtears rather than inflammatory cell infiltration.
Classic clinical features include:
When a patient’s presentation deviates from this pattern — or fails to improve after 6–12 weeks of appropriate management — it should prompt us to reconsider the diagnosis.
Heel Pain That Mimics Plantar Fasciitis
1. Heel Fat Pad Syndrome
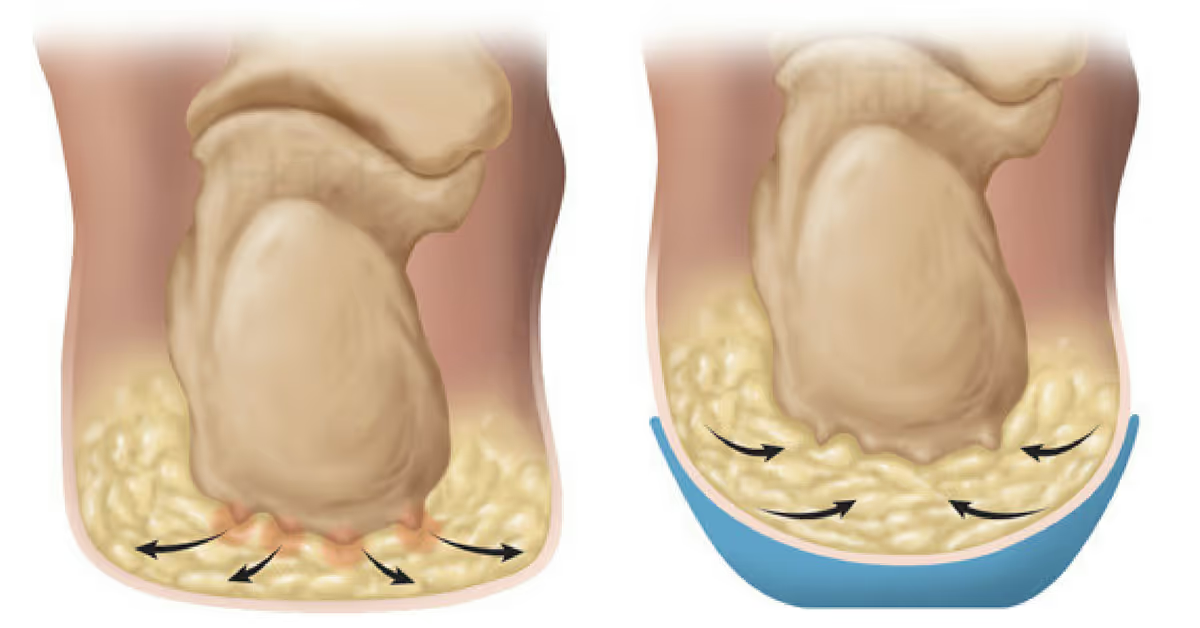
Frequently overlooked, heel fat pad syndrome presents with:
Age-related fat pad atrophy, repetitive impact, or corticosteroid injections may contribute. Importantly, treatment focuses on cushioning and load modification, not plantar fascia stretching.
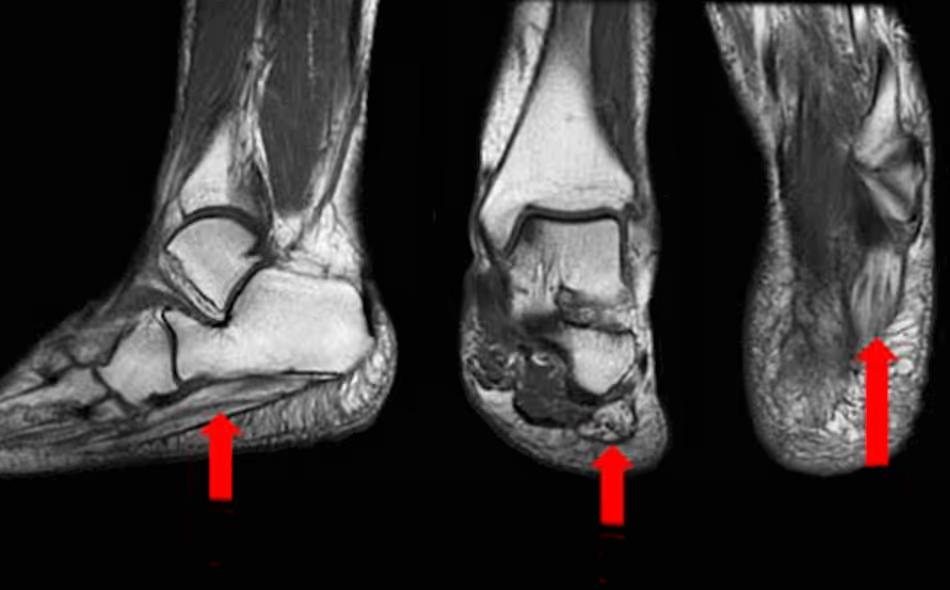
2. Calcaneal Stress Fracture
Stress fractures of the calcaneus should be suspected when:

Plain radiographs may be normal early on, making MRI the preferred diagnostic modality. Continued weight-bearing under the assumption of plantar fasciitis can significantly delay healing.
3. Baxter’s Nerve Entrapment (Inferior Calcaneal Neuropathy)
This condition can account for up to 20% of chronic heel pain cases and is commonly misdiagnosed.
Clinical clues include:
Neuropathic pain characteristics should always prompt consideration of nerve involvement.
4. Achilles Tendinopathy and Retrocalcaneal Bursitis
Posterior heel pain is often mistakenly grouped under “heel pain” broadly, yet:
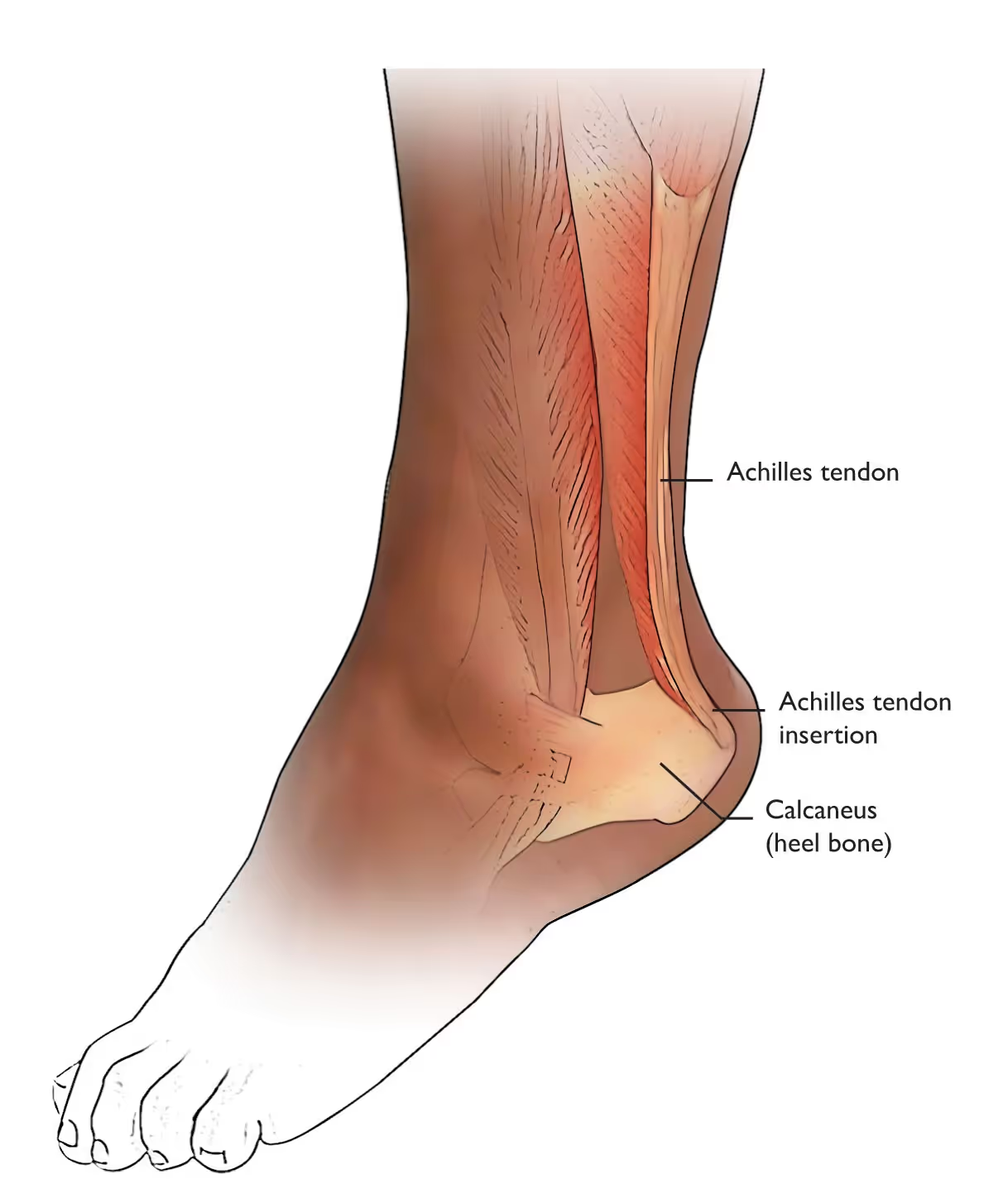
These findings point away from plantar fasciitis and toward posterior heel pathology.
5. Inflammatory and Systemic Causes
Bilateral heel pain, especially in younger patients or those with morning stiffness lasting over 30 minutes, should raise suspicion for:
Heel pain can be an early enthesopathic manifestation of systemic disease.
Why Accurate Diagnosis Matters
Plantar fasciitis protocols emphasize:
However, these interventions may be ineffective or harmful when applied to:



Comments
Post a Comment